Strengths and limitations of this study
-
The study used a nationally representative survey sample of older adults.
-
This is the first study in India that looked into the amount of time spent in physical activities by older adults in India.
-
Due to the cross-sectional nature of the study design, the present study could not establish a causal relation.
-
The study has used a comprehensive list of potentially confounding variables.
-
The reporting of any morbidity and physical activity was based on the individual’s self-reporting information, and hence there is the possibility of reporting biases and underestimation as well.
Introduction
Co-occurrence of two or more chronic health conditions in an individual (any one of which should be a long-term physical non-communicable disease or a mental health condition of long duration or a long-term infectious illness)1 is known as multimorbidity, a rapidly growing concern in public health.2 Multimorbidity at older ages is associated with unhealthy lifestyles.3 4 It is also found to have adverse effects on quality of life, mortality rates, functional health, psychological health, cognitive health and healthcare expenditure.5–8 Physical activity is recommended as one of the leading lifestyle changes in preventing and managing multiple chronic diseases worldwide.9 While some previous studies depicted the high burden of multimorbidity due to physical inactivity,10 11 other studies showed no association between physical activity and multimorbidity.4 12
Physical activity (PA) is defined as any bodily movement produced by skeletal muscles that result in energy expenditure, including daily activities like playing, carrying out of household chores, travelling and activities during professional and recreational pursuits.13 Regular PA is associated with increased life expectancy and reduced risk of coronary heart disease, heart stroke, diabetes, hypertension and obesity.14 PA not only helps in the prevention and management of many risk factors, chronic diseases like cardiovascular disease, colon and breast cancer, diabetes and obesity, and functional disabilities associated with old age, but it may may decrease the period of disability at the end of life.15 16 PA declines proportionately with age among older adults.17 Despite their knowledge about the potential personal benefits of participating in PAs, many adults hardly engage in them.18
Along with the rise in ageing populations in Asian countries, South Asia is also experiencing a growing burden of multimorbidity among the ageing population. The risk factors are mainly due to lifestyle factors such as diet and inactivity.19 20 In India, more than half of the burden of non-communicable diseases occurred in the 45+ age group.21 A study found that multimorbidity was 23% in the pooled sample of six countries—the highest being in Russia (35%), followed by Mexico (27%), India (24%), Ghana (23%), South Africa (32%) and China (20%).22 According to another study in India, 30.6% of adults aged 70 and above reported more than one chronic condition, while only 1.3% of respondents between 18 and 29 reported the same in comparison.23 Therefore, India faces a high burden of non-communicable diseases due to rapid urbanisation.24 Looking at the growing concern on multimorbidity in India, there is the necessity for a better understanding of the epidemiology of multimorbidity and the risk factors contributing to it. Studies have primarily examined the association between multimorbidity and socioeconomic status in India.25 PA among older adults is a popular area of research, especially in low-income or middle-income countries of South Asia, where the population demographics are fast changing.26 However, the relationship between multimorbidity and PA levels remains poorly documented among older adults, especially in India, due to the lack of available data. A better understanding of this relationship would facilitate the development of more appropriate action to combat the burden of multimorbidity.
Thus, the current study has aimed to examine the effects of PA on multimorbidity after controlling the role of other socio-demographic factors among older adults aged 45 and above in India.
Methods
Study population
The study used data from the WAVE 1 of the Longitudinal Ageing Survey in India (LASI) data.27 It is a nationally representative survey of 72 250 older adults aged 45 and above, and their spouses irrespective of their ages, including 31 464 elderly aged 60 and above and 6749 oldest-old persons aged 75 and above from 35 states and union territories of India (excluding Sikkim).28 The data were collected during the year 2017–2018. It is a full-scale national survey of scientific investigation of India’s health, economics and social determinants and consequences of population ageing. The LASI is envisioned to be conducted every 2 years for the next 25 years. It is the world’s most extensive and India’s first longitudinal ageing study. The LASI has adopted a multistage stratified area probability cluster sampling design to select its required sample.28
In this study, individuals below the age of 45 have been excluded. After dropping, a lot of missing values, the study has a total sample of 65 336 aged 45 and above. Considering the age group of 45–59 years is essential to study ageing and health transition from prime adult ages as it represents pre-ageing and pre-retirement phases. The details of the study design, sampling procedure and data collection methods can be obtained from the official report of LASI.28
Variable description
Dependent variable
A score was calculated from the 12 morbidities reported by the participants. It was then categorised into 2=multimorbidity, 1=one morbidity and 0=none. The question asked for each of the illnesses was, ‘Has any health professional ever told you that you have a (particular) disease?’ and each response was coded as yes and no.28 The morbidities reported are shown in the online supplemental appendix list.
Supplemental material
Explanatory variables
Self-reported questionnaires were used in a face-to-face interview where responses were recorded with the help of computer-assisted personal interviews. The questions were asked separately for both moderate and vigorous PAs. The development of the PA indicators were based on the WHO Global recommendations.29Before the survey was carried, the LASI pilot survey was done successfully in 2010.30
The calculation of the weekly time devoted to PA for each surveyed individual was based on metabolic equivalent tasks (METs), which reflects the estimates of the ratio of energy expended during a particular PA to energy expended while sitting quietly. The number of weekly hours and minutes a subject dedicated to each type of activity was multiplied by the MET value, that is, moderate (four METs) and vigorous (eight METs) PAs assigned to that activity based on the International Physical Activity Questionnaire criteria.31 Total PA scores in MET min/week were calculated by summing the MET values. The MET values of moderate and vigorous PA were finally categorised separately into 0 (never involved), low <599 MET-min/week), moderate (600–1499 MET-min/week) and high (≥1500 MET-min/week). The question through which PA was assessed was ‘How often do you take part in moderate physical activities such as cleaning the house, washing clothes by hand, fetching water or wood, drawing water from a well, gardening, bicycling regularly, walking at a moderate pace, dancing, floor or stretching exercises (everyday, more than once a week, once a week, one to three times a month or hardly ever or never)?’. If the respondents reported yes, then the question ‘How much time did you usually spend doing any moderate activity on an average in a day’ was asked.27
A similar question was asked for vigorous PAs: ‘How often do you take part in sports or vigorous activities, such as running or jogging, swimming, going to a health center or gym, cycling, digging with a spade or shovel, heavy lifting, chopping, farm work, fast cycling, cycling with loads (everyday, more than once a week, once a week, one to three times a month, hardly ever or never)’. The second question asked for those reporting yes ‘On the days you did any vigorous activity, how much time did you usually spend doing it?’.27
Other explanatory variables
The demographic and socioeconomic variables considered for this study are sex (male and female), place of residence (rural and urban), marital status (currently married, widowed/divorced/separated and never married), education (illiterate, primary, secondary, higher secondary and above), work status was categorised as working, retired and not working.Living arrangement was categorised as living alone, living with spouse and others, living without spouse and others.The age group was classified as (45–59, 60–74, 75 and above). The monthly per capita expenditure (MPCE) quintile was measured using household consumption data. Sets of 11 and 29 questions on the spending on food and non-food items, respectively, were used to canvas the sample households. The variable was then divided into five quintiles, that is, from poorest to richest. Religion was categorised as Hindu, Muslim and Others, the social groups as Scheduled Castes(SC), Scheduled Tribes (ST), Other Backward Classes(OBC) and others. \.
Patient and public involvement
No patients were involved in this study.
Statistical analysis
Bivariate analysis was presented to show the association between multimorbidity and other covariates. Multinomial logistic regression analyses were used to examine the extent to which vigorous and moderate PA level was associated with multimorbidity. The first model was run to investigate the association between moderate PA level and multimorbidity. The second model was run to examine the association between vigorous PA level and multimorbidity. The third model was statistically adjusted for other demographic and socioeconomic factors.
Results
Table 1 presents the weighted characteristics of the study sample by morbidity status, the total sample and its percentage. Out of 65 336 participants, 29.61% had one morbidity and 27.39% had multimorbidity. The prevalence of one morbidity and multimorbidity increased from younger to the older age groups. Female older adults had a higher share in multimorbidity (28.93%) than men (25.57%). The older adults living in urban areas had a higher prevalence of multimorbidity (36.43%) than those living in rural areas (23.27%). Older adults from ST (13.51%) had the lowest prevalence of multimorbidity among all the caste groups, and Hindus (26.17%) had the lowest among religions. About 30.44% of older adults who were widowed, divorced or separated suffered from multimorbidity. The multimorbidity status among older adults showed an increasing trend with a rising MPCE quintile. The working older adults had the lowest prevalence of multimorbidity (18.9%) compared with those who had never worked and who had worked before.
Demographic and socioeconomic characteristics for older adults (aged 45+ years) in India, LASI (2017–2018)
The proportion of older adults with increasing moderate PA levels had a lower prevalence of multimorbidity. The older adults who were never engaged and with a low level of PA had a higher prevalence of multimorbidity, that is, 29.83% and 27.99%. Similarly, the older adults involved in a high level of vigorous PA had the lowest prevalence of multimorbidity (19.69%). In comparison, those who never engaged in vigorous activities had the highest prevalence of multimorbidity (31.68%).
Figure 1 presents the distribution of moderate PA of older adults by age group. The percentage of older adults who were never involved in moderate PA was the highest for the age 75 and above (57.37%) and lowest for 45–59 (23.13%). All moderate PA levels were highest for the individuals aged 45–59 and the lowest for the age group 75 and above. The highest difference was observed for a high level of moderate PA where for the age group 45–59 it was 52.16% and for 75 and above it was only 21.41%.

Percentage distribution of older adults engaged in moderate physical activities by age groups in India,LASI (2017–2018).
Figure 2 presents the distribution of older adults engaged in different vigorous activity levels. The older adults who never engaged in any vigorous activities were highest for the age group 75 and above that is, 84.13%, while it was lowest for those aged 45–59 (49.64%). The percentage of older adults aged 75 and above was lowest in all kinds of vigorous PA levels while it was highest for 45–59.
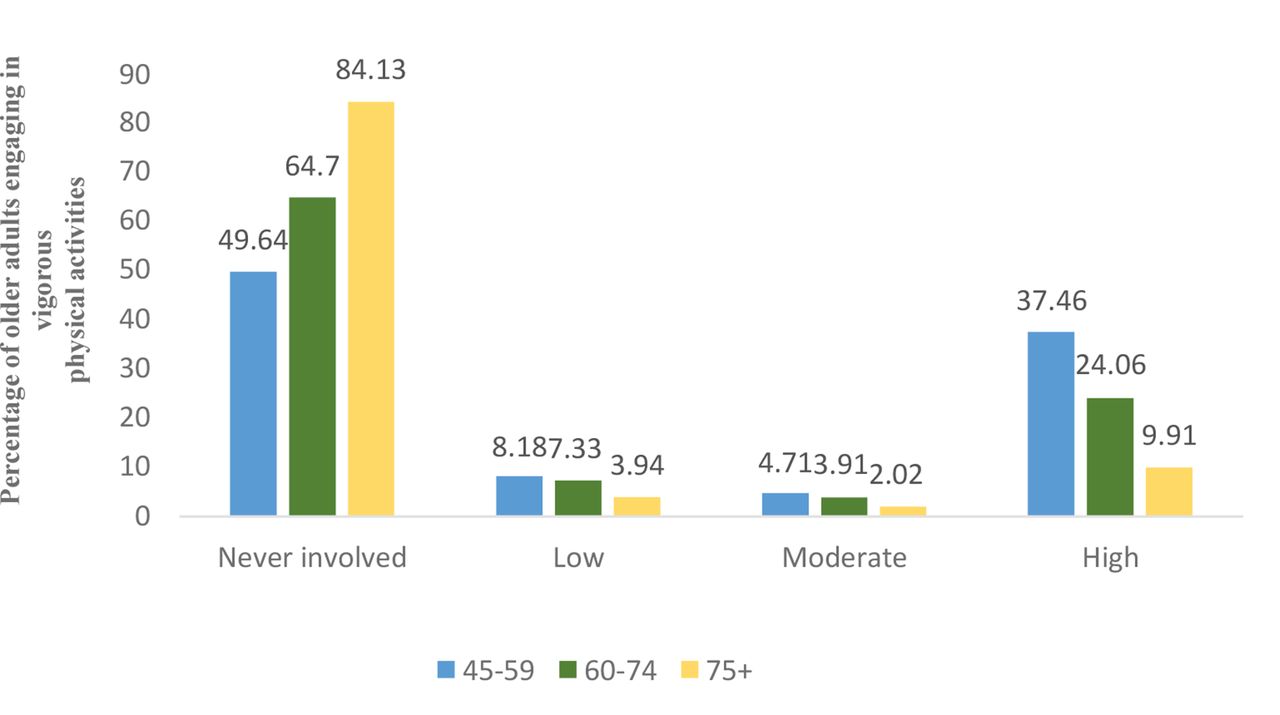
Percentage distribution of older adults engaged in vigorous physical activities by age groups in India, LASI (2017–2018).
Table 2 shows the results of the multinomial logistic regression models on multimorbidity. Model 1 presents the association of multimorbidity and moderate PA level for older adults. It was found that older adults who were engaged in a high level of moderate PA were significantly less likely to have one morbidity in comparison with those who were never engaged in any (unadjusted relative risk ratio (UA RRR)): 0.95, 95% CI 0.91 to 0.99). On the other hand, the RRR of multimorbidity was significantly lower for older adults engaged in high, moderate and low levels of moderate PA level than those who were never involved.
Logistic regression estimates for the prevalence of multimorbidity among older adults aged 45 years and above, Longitudinal Ageing Survey in India (2017–2018)
Model 2 shows the association of multimorbidity and vigorous PA level for older adults. For vigorous activity level, the prevalence of multimorbidity was significantly less likely for those engaging in high level than those who were never involved (UN RRR 0.44; 95% CI –0.42 to 0.46). Similarly, the older adults who engaged in moderate PA level (UN RRR 0.59; 95% CI –0.54 to 0.65) and low vigorous PA level (UN RRR 0.72; 95% CI –0.67 to 0.77) were also significantly less likely to report multimorbidity than those who never engaged. The results for one morbidity showed similar results with multimorbidity, where the likelihood of having one morbidity decreased significantly with vigorous PA level. Model 3 shows the association of multimorbidity and for both moderate and vigorous PA levels for older adults for sex, age, residence, educational status, caste, religion, marital status, living arrangements, work status and wealth quintile. The results from the adjusted model suggest that the older adults who were engaged in moderate (adjusted RRR (A RRR)=1.10; 95% CI 1.03 to 1.18) and low levels of moderate PA (A RRR=1.05; 95% CI 0.98 to 1.13) were significantly more likely to have multimorbidity. The results showed the same for one morbidity also. However, the older adults who were engaged in all kinds of vigorous PA were significantly less likely to have multimorbidity. In the case of one morbidity, only those engaging in a high level of vigorous activity were significantly less likely to have multimorbidity.
Discussion
Using LASI data on older adults, this study has found 27.39% of older adults in India to have multimorbidity. To our knowledge, the present study is the first attempt in India to investigate the association between multimorbidity and the level of PA among older adults aged 45 and above. In this analysis of older adults, our study depicts an inverse association between multimorbidity and PA level for both moderate and vigorous activity. Results suggest that a higher level of PA significantly lowers the likelihood of multimorbidity among older adults. Our findings are consistent with a study that demonstrated an inverse dose-response association between PA levels and multimorbidity using frequency of vigorous, moderate and mild PA.32 In another study for older adults aged 65 and above, it was found that the absence of 13 chronic conditions was associated with those who engaged in moderate-intensity PA lasting 15 min per day at least three times a week10
The study also found that multimorbidity was inversely associated with PA among older adults after controlling for sex, age, residence, educational status, caste, religion, marital status, living arrangements, work status and wealth quintile. Similar results were found in another study where multimorbidity was inversely associated with PA in the youngest and oldest age groups after controlling for long-term activity limitations, self-perceived health status, age, sex, educational level and employment status.33 However, the likelihood of multimorbidity increased with the level of moderate PA after adjusting with the other covariates, which needs further investigation. The findings of this study are in concordance with existing literature that women and older age groups tend to have a higher prevalence of multimorbidity.3 25 34 35 Older age groups having a higher rate of multimorbidity than the younger age groups might be explained due to the fact that susceptibility to stressful events throughout a lifetime disrupts the physiological balance and hence expedites the onset of morbid conditions36
Moreover, the study has also documented the higher prevalence of multimorbidity among the higher socioeconomic groups, which is also consistent with other studies in India.22 26 27 Those residing in urban areas, higher education status, the wealthiest, the high caste groups were more likely to have multimorbidity. This may be explained due to the adoption of unhealthy lifestyles among the higher socioeconomic groups leading to obesity, high-risk waist-hip ratio and elevated lipids, which are also major risk factors of morbidity conditions.37 38 Additionally, self-report-based results of the low prevalence of multimorbidity among less educated and poor older persons are likely to have a substantial burden of undiagnosed chronic diseases.34
The present study has several limitations, including its cross-sectional design, which cannot establish a causal inference between multimorbidity and time use in PAs. The reporting of any morbid condition was based on self-reported information, and hence there is the possibility of reporting bias and underestimation as well. Some respondents might not have had the disease due to treatment at the time of the survey, and some might not have consulted any medical professional. Moreover, the data on PA might have errors due to recall and reporting biases.
Conclusion
The present study found a negative association between PA and multimorbidity in older adults. Older adults spending more time in vigorous activities had lower odds of multimorbidity. The WHO recommends that older adults should do at least 150 min of moderate-intensity PA during the week or at least 75 min of vigorous-intensity PA during the week or an equivalent combination of both.9 Therefore, the promotion of PA should be adopted as a primary strategy in reducing the burden of morbidity and multimorbidity.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
This post was originally published on https://bmjopen.bmj.com