STRENGTHS AND LIMITATIONS OF THIS STUDY
-
This is a large observational cohort study in a single integrated health system.
-
We applied inverse probability of treatment weighting to account for limitations which resulted in well balanced treated versus non-treated groups.
-
Tocilizumab-treated and non-tocilizumab-treated patients were characteristically different.
-
Confounding associated with unmeasured treatment practices might have improved overall survival after the initial 6 months of the pandemic.
Background
Patients who receive invasive mechanical ventilation for COVID-19 are at increased risk of mortality. For this high-risk group of patients with COVID-19, few therapies have been shown to reduce mortality or improve outcomes. Treatments targeting the host immune response to infection have been proposed to potentially diminish inflammation and improve outcomes.1 In addition to systemic corticosteroids, tocilizumab, a humanised monoclonal antibody against the interleukin 6 (IL-6) receptor, has been evaluated as a potential therapy in both randomised controlled trials and observational analyses.2–14 On 25 June 2021, the US Food and Drug Administration issued an Emergency Use Authorisation for the use of tocilizumab for the treatment of COVID-19 in hospitalised persons aged ≥2 years who are receiving systemic corticosteroids and require supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO).15
In a meta-analysis of 27 clinical trials assessing the association between receipt of IL-6 antagonists and mortality among patients hospitalised with COVID-19, patients who received an IL-6 antagonist had significantly lower 28-day mortality.2 However, of the 8050 patients included in the meta-analysis, only 1211 (15%) were receiving invasive mechanical ventilation at the time of randomisation and in this subgroup the receipt of IL-6 antagonists was not associated with reduced mortality. To provide additional data to address the potential efficacy of tocilizumab to improve outcomes among mechanically ventilated patients with COVID-19, we conducted this observational analysis using a target trial emulation approach. Data from a large integrated health system were used to estimate the effect of treatment with tocilizumab on time to death, extubation and discharge in mechanically ventilated patients with COVID-19.
Methods
Study design
We emulated a hypothetical target trial in which mechanically ventilated adults with COVID-19 received or did not receive tocilizumab after initiation of invasive mechanical ventilation with predefined outcomes of death, time to extubation and time to hospital discharge over a 28-day follow-up period. We identified a cohort of patients with COVID-19 who required mechanical ventilation from two regions of a large integrated health system, Kaiser Permanente Northern California and Kaiser Permanente Southern California. The main exposure of interest was receipt of tocilizumab within 10 days of initiation of mechanical ventilation. Data were extracted from Kaiser Permanente administrative databases and from an integrated electronic health record database (Epic, Verona, Wisconsin, USA). This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline. It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Eligibility criteria
We included adult patients (aged ≥18 years) with laboratory-confirmed COVID-19 who required invasive mechanical ventilation from 1 March 2020 to 31 January 2021. To meet inclusion criteria, patients had to have SARS-CoV-2 detected by PCR testing of a nasopharyngeal or oropharyngeal specimen in the 14 days prior to hospitalisation or during hospitalisation and require hospitalisation for COVID-19 pneumonia. Invasive mechanical ventilation was defined as the delivery of positive pressure to the lungs via an endotracheal or tracheostomy tube. We applied the following exclusion criteria as assessed at the time of initiation of mechanical ventilation to exclude patients who would not be eligible to receive tocilizumab in a clinical trial: pregnant or breast feeding in the prior 6 months, recorded allergy to tocilizumab, history of organ transplantation, alanine transaminase or aspartate aminotransferase >10 times the upper limit normal, absolute neutrophil count <1000/mm3 or platelet count <50 000/µL. We also excluded patients who received tocilizumab prior to initiation of mechanical ventilation, who received an IL-6 antagonist other than tocilizumab or who died within 24 hours of initiation of mechanical ventilation.
Treatment strategies
Patients were categorised according to whether they received or did not receive tocilizumab in the first 10 days after initiation of mechanical ventilation. All tocilizumab administration was based on the discretion of the treating clinician; no active clinical trials or institutional guidelines recommended tocilizumab use. Ten days was chosen to capture a diversity of patients who received tocilizumab in Kaiser Permanente in California, USA. Exposure to tocilizumab was defined as a time-dependent variable and thus patients who received tocilizumab on days 0–10 after initiation of mechanical ventilation were in the non-tocilizumab-treated group until the day of tocilizumab treatment. Patients who received tocilizumab more than 10 days after initiation of mechanical ventilation were categorised in the non-tocilizumab-treated group and censored on the day of tocilizumab receipt (n=14).
Statistical analysis
Overview
We followed patients until death or 28 days after intubation, whichever occurred first, for the primary analysis examining the hazard of death in relation to tocilizumab treatment. A 28-day follow-up period has been commonly used in randomised controlled trials of IL-6 inhibitors for treatment of COVID-19. The secondary analyses examined time to extubation from mechanical ventilation and time to hospital discharge in relation to tocilizumab treatment; note deceased patients were followed to day 28 to account for the competing risk of death in these analyses. Adjusted hazard ratios (aHRs) and 95% CIs were estimated using Cox regression.
To adjust for confounding we used inverse probability of treatment weighting (IPTW). Using site-specific (Northern California and Southern California) logistic regression models, we calculated propensity scores, estimating the propensity to receive tocilizumab in relation to the following prespecified covariates based on literature review for established risk factors for severe COVID-19 outcomes that were available in our dataset: age, sex, race/ethnicity, body mass index, diabetes, hypertension, Charlson Comorbidity Index score,16 median vital signs on initiation of mechanical ventilation (maximum temperature, systolic blood pressure, diastolic blood pressure, heart rate, respiratory rate), month of enrolment, median days from hospital admission to initiation of mechanical ventilation and receipt of remdesivir, corticosteroids or COVID-19 convalescent plasma. We used the propensity scores to calculate weights targeting average treatment effects for the treated. Models for outcomes were not only IPTW weighted, they also included covariates for study site, index month, sex, age, race/ethnicity, body mass index and time dependent variables for receipt of COVID-19 specific treatments (remdesivir, corticosteroids, COVID-19 convalescent plasma) to account for the receipt of those treatments either before or after initiation of mechanical ventilation. In addition, receipt of tocilizumab was specified as a time dependent variable to account for the time between initiation of mechanical ventilation and receipt of tocilizumab.
Subgroup and sensitivity analyses
We used similar methods as in the primary and secondary analyses to assess the effect of tocilizumab in three predefined subgroups: days from initiation of mechanical ventilation to receipt of tocilizumab (tocilizumab received on days 0–2 vs tocilizumab received on days 3–10), age group (<60 vs ≥60 years) and receipt of corticosteroids (received corticosteroids vs did not receive corticosteroids). In addition, we conducted a sensitivity analysis in which we matched tocilizumab-treated patients with non-tocilizumab-treated patients based on the same propensity scores used to compute the inverse probability weights. A 1:1 optimal matching algorithm was employed with a calliper on the linear propensity score of 0.25 SD and an exact match on site. We then replicated the final Cox regression model adjusting for the same confounders as in the IPW model above, but also including maximum temperature since the propensity score match yielded a standardised difference >0.20. All analyses described above were performed using SAS software, V.9.4 (SAS Institute).
Missing data
To keep all eligible patients, we imputed missing values for the following variables: body mass index (67; 1.6%), maximum temperature (34; 0.8%), systolic blood pressure (34; 0.8%), diastolic blood pressure (34; 0.8%), heart rate (33; 0.8%) and respiratory rate (31; 0.7%), using R package Multiple Imputation by Chained Equations.17 18
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
We identified 4446 patients hospitalised with COVID-19 who required invasive mechanical ventilation during their initial hospitalisation from 1 March 2020 to 31 January 2021 (figure 1). Of these, 261 met exclusion criteria and thus 4185 patients were included in the primary analysis; 184 (4.4%) who received tocilizumab in the first 10 days after initiation of mechanical ventilation and 4001 (95.6%) who did not receive tocilizumab within the first 10 days after initiation of mechanical ventilation. Demographic, clinical and treatment characteristics of patients who received tocilizumab and those who did not receive tocilizumab before and after IPTW weighting are presented in table 1.
Demographic, clinical and treatment characteristics of patients before and after applying inverse probability treatment weights (IPTW)

Study cohort and emulated trial flow.
Tocilizumab-treated patients were younger (median age, 59.5 (IQR 53–68) vs 64 (IQR 55–72) years, more likely to be male (77.7% vs 66.4%), equally likely to be obese (median BMI 31.0 vs 31.0), less likely to have diabetes (49.5% vs 53.4%) or hypertension (59.2% vs 65.1%), less likely to have comorbidities (median Charlson score 1.0 vs 2.0), and more likely to have been hospitalised in March–April 2020 (56.0% vs 9.0%) rather than November 2020–January 2021 (12.0% vs 65.1%) compared with non-tocilizumab-treated patients. In addition, tocilizumab-treated patients were less likely to receive remdesivir (27.2% vs 61.0%), corticosteroids (38.6% vs 74.1%) and COVID-19 convalescent plasma (7.1% vs 17.3%) compared with non-tocilizumab-treated patients.
After applying weights, demographic, clinical and treatment characteristics were well balanced between the groups and the standardised differences between the tocilizumab and non-tocilizumab groups were <0.20 for all covariates. Of note, both weighted groups included 27% who received remdesivir, 38% who received corticosteroids and 7% who received COVID-19 convalescent plasma.
Among the 4185 patients included in this analysis, the median follow-up for tocilizumab-treated patients was 28.0 (IQR 28.0–28.0) and non-tocilizumab-treated patients was 28.0 (IQR 28.0–28.0) days. A total of 862 patients (20.6%) were discharged alive, 2485 (59.4%) died and 838 (20.0%) remained hospitalised at day 28. A total of 2485 patients who died included 86 of the 184 (46.7%) tocilizumab-treated patients and 2399 of the 4001 (60.0%) non-tocilizumab-treated patients (table 2).
Overall, subgroup and sensitivity analyses examining mortality, time to extubation from mechanical ventilation and hospital discharge in tocilizumab-treated versus non-tocilizumab-treated patients
In the primary analysis, after adjusting for confounding, tocilizumab-treated patients had a similar risk of mortality (aHR 1.21; 95% CI 0.98 to 1.50) than non-tocilizumab-treated patients (figure 2). However, tocilizumab-treated patients had a significantly longer time-to-extubation (aHR 0.71; 95% CI 0.57 to 0.88) and time-to-hospital-discharge (aHR 0.66; 95% CI 0.50 to 0.88) in comparison with non-tocilizumab-treated patients. The 28-day weighted cumulative incidence of mortality was 46.7% (95% CI 39.8% to 54.2%) in the tocilizumab-treated patients and 40.3% (95% CI 36.8% to 44.0%) in the non-tocilizumab-treated patients (risk difference 6.4%; 95% CI −1.0% to 13.8%) (figure 3). Similarly, the 28-day weighted cumulative incidence of extubation from mechanical ventilation was 63.0% (95% CI 54.1% to 71.9%) in the tocilizumab-treated patients and 68.6% (95% CI 64.4% to 72.7%) in the non-tocilizumab-treated patients (risk difference −5.6%; 95% CI −12.7% to 1.6%) and the 28-day weighted cumulative incidence of hospital discharge was 44.8% (95% CI 35.8% to 54.8%) in the tocilizumab-treated patients and 47.5% (95% CI 43.0% to 52.3%) in the non-tocilizumab-treated patients (risk difference −2.7%; 95% CI −10.1% to 4.6%).

Overall, subgroup and sensitivity analyses examining adjusted risk of mortality, time to extubation from mechanical ventilation and hospital discharge in tocilizumab-treated versus non-tocilizumab-treated patients.
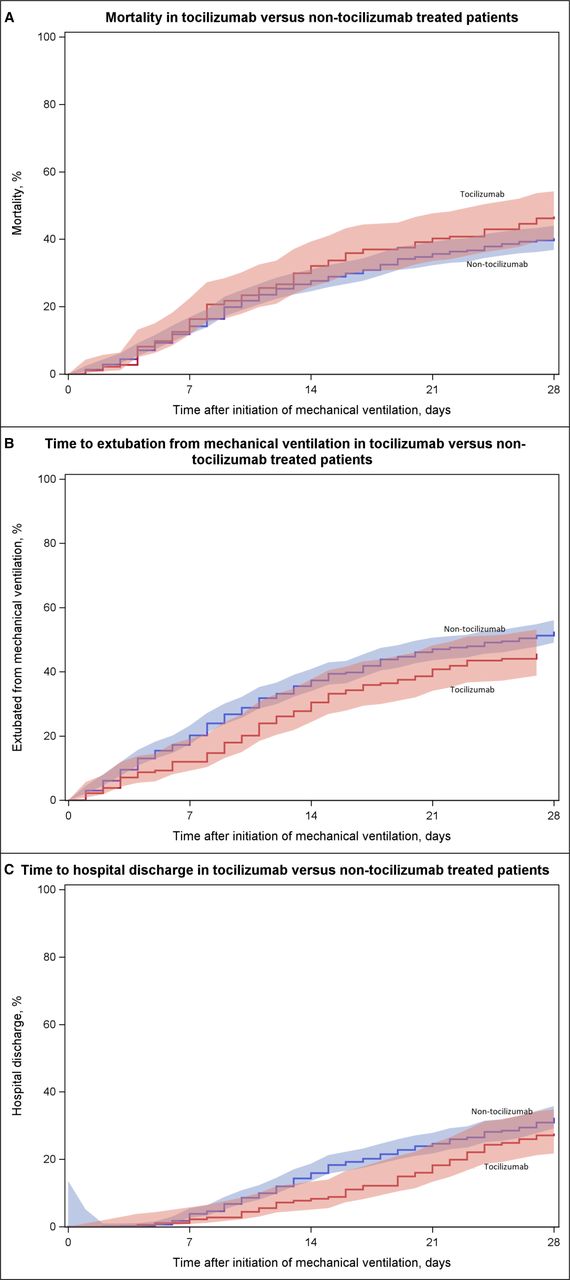
Cumulative incidence of mortality (A), extubation from mechanical ventilation (B), and hospital discharge (C) in inverse probability weighted tocilizumab-treated vs non-tocilizumab-treated patients.
In the three subgroup analyses, tocilizumab-treated patients who received tocilizumab 3–10 days after initiation of mechanical ventilation (aHR 1.59; 95% CI 1.18 to 2.15), were aged <60 years (aHR 1.52; 95% CI 1.10 to 2.11) or used corticosteroids (aHR 1.43; 95% CI 1.14 to 1.79) had a significantly increased risk of mortality compared with non-tocilizumab-treated patients (table 2). Similarly, tocilizumab-treated patients who received tocilizumab 3–10 days after initiation of mechanical ventilation (aHR 0.36; 95% CI 0.22 to 0.61), were aged <60 years (aHR 0.52; 95% CI 0.36 to 0.77) or used corticosteroids (aHR 0.49; 95% CI 0.33 to 0.72) had significantly longer time-to-hospital-discharge compared with non-tocilizumab-treated patients. In the sensitivity analysis using 1:1 propensity score matching to compare tocilizumab-treated versus non-tocilizumab-treated patients, tocilizumab-treated patients had an increased risk of mortality compared with non-tocilizumab-treated patients (aHR 1.70; 95% CI 1.21 to 2.38). Patients treated with tocilizumab ≤2 days after initiation of mechanical ventilation had a similar risk of mortality (aHR 1.47; 95% CI 0.96 to 2.26), but significantly shorter time-to-extubation (aHR 0.37; 95% CI 0.23 to 0.58) and time-to-hospital-discharge (aHR 0.31; 95% CI 0.17 to 0.56) compared with patients treated with tocilizumab 3–10 days after initiation of mechanical ventilation.
Crude mortality was lower among tocilizumab-treated patients (46.7%) than non-tocilizumab-treated patients (60.0%), but after applying IPTW and adjusting for confounding, tocilizumab-treated patients had a similar risk of mortality than non-tocilizumab-treated patients (aHR 1.21; 95% CI 0.98 to 1.50). To assess whether the risk of death associated with receipt of tocilizumab was related to time period of treatment (March 2020 to August 2020 vs September 2020 to January 2021), we conducted an analysis stratified by time period. In this analysis, crude mortality was 43.1% among tocilizumab-treated patients vs 44.3% in non-tocilizumab-treated patients in March to August 2020 and 70.8% among tocilizumab-treated patients vs 66.6% in non-tocilizumab-treated patients in September 2020 to January 2021 (online supplemental tables 1 and 2; online supplemental figure 1).
Supplemental material
Discussion
In this study of 4185 mechanically ventilated patients with COVID-19 hospitalised in 36 hospitals in a large integrated health system in California, USA, patients treated with tocilizumab in the first 10 days after initiation of mechanical ventilation had a similar risk of death within 28 days compared with non-tocilizumab-treated patients, but had a significantly longer time-to-extubation from mechanical ventilation and longer time-to-hospital discharge.
Tocilizumab has been studied extensively for the treatment of patients hospitalised with COVID-19. In a meta-analysis of 19 clinical trials, the receipt of tocilizumab was associated with reduced 28-day mortality among all hospitalised patients, but not the subgroup of patients who were on invasive mechanical ventilation or ECMO at the time of randomisation.2 This observational study found a similar risk of death in patients who received tocilizumab 0–10 days after initiation of mechanical ventilation, but a longer time-to-extubation and time-to-hospital discharge. Thus, both the composite clinical trial data as well as this study suggest caution in using tocilizumab in critically ill patients who are on mechanical ventilation. The current National Institutes of Health and Infectious Diseases Society of America guidelines as well as the US Food and Drug Administration Emergency Use Authorisation for tocilizumab currently recommend use in mechanically ventilated patients within the first 24 hours of initiation of mechanical ventilation,15 19 20 but additional clinical trials are needed to clearly define the role of tocilizumab in patients in this critically ill, high-risk population.
The association between tocilizumab administration and reduced mortality might be dependent on timing of administration after initiation of mechanical ventilation. Other studies suggest that earlier administration might be beneficial2 11 and our understanding of the proinflammatory response to severe COVID-19 suggests that there might be a specific therapeutic window to blunt the inflammatory response to affect clinical trajectories.21 In this study, the risk of death was significantly increased in the subgroup of patients who received tocilizumab 3–10 days after initiation of mechanical ventilation but was not significantly increased in the subgroup of patients who received tocilizumab on days ≤2 after initiation of mechanical ventilation further supporting the theory that timing of tocilizumab administration is an important factor in the use of tocilizumab for the treatment of severe COVID-19 pneumonia. Future studies should address the timing of tocilizumab administration in relationship to initiation of mechanical ventilation to better understand how to optimally use tocilizumab.
Current guidelines based on existing evidence support the concurrent use of tocilizumab and corticosteroids.19 20 Prior studies suggest that patients treated with corticosteroids and tocilizumab had reduced mortality compared with patients treated with corticosteroids alone.3 11 However, we found increased mortality in the subgroup of patients treated with both tocilizumab and corticosteroids in the full analysis that included patients who received tocilizumab within 10 days of initiation of mechanical ventilation. It is unclear whether this finding is due to residual confounding, changing treatment practices over time or other factors. Data on treatment for mechanically ventilated patients with COVID-19 are scarce, and thus as suggested by others future studies will need to reassess the concurrent use of tocilizumab and corticosteroids.21
This analysis has several strengths. First, our entire large cohort was enrolled in a single large integrated health system with similar clinical treatment guidelines and practices using standardised abstraction methods to extract data from the electronic medical record. Second, we use methods that emulate a target clinical trial and analytic approaches to adjust for confounding by indication and prevent immortal time bias. Third, we used both IPTW and multivariate Cox models to doubly adjust for potential imbalance between the tocilizumab-treated and non-tocilizumab-treated groups. Fourth, we adjusted for concomitant treatment with remdesivir, corticosteroids and COVID-19 convalescent plasma as time dependent covariates to adjust for exposure to these treatments.
This study has limitations. First, the tocilizumab-treated and the non-tocilizumab-treated groups differed substantially before applying IPTW with tocilizumab-treated patients more likely to be younger, male and enrolled earlier during the pandemic (eg, March–August 2020), but less likely to have been treated with remdesivir, corticosteroids or COVID-19 convalescent plasma. In particular, we were concerned about confounding associated with unmeasured treatment practices that might have improved overall survival after the initial 6 months of the pandemic. To address this concern, we conducted a stratified analysis and noted that receipt of tocilizumab was associated with increased crude mortality in both time periods March to August 2020 and September 2020 to January 2021. Note that after applying IPTW the demographic, clinical and treatment characteristics as well as time period of enrolment were all well balanced between the tocilizumab-treated and non-tocilizumab-treated groups and thus expect to have accounted for the effect of time period in our analyses. However, as a retrospective study, even though, we used IPTW and multivariate Cox regression to doubly adjust for potential imbalance between the tocilizumab-treated and non-tocilizumab-treated groups, there is still potential for residual confounding. Second, we did not collect data on all possible confounders and thus there might be additional confounding from unmeasured differences between the patients who did or did not receive tocilizumab, including confounding by indication.
Among mechanically ventilated patients with COVID-19, patients treated with tocilizumab in the first 10 days after initiation of mechanical ventilation had a similar risk of mortality, but a longer time-to-extubation and time-to-hospital-discharge compared with patients not treated with tocilizumab. These findings may be susceptible to unmeasured confounding and thus additional randomised controlled trials of tocilizumab treatment in mechanically ventilated patients with COVID-19 are needed to establish the role of tocilizumab treatment in this population of COVID-19 patients at highest risk of mortality.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by 1588244, Kaiser Permanente Southern CA Institutional Review Board, with waivers of the requirement for informed consent.
Acknowledgments
The authors are grateful to all Kaiser members without whom this study would not have been possible.
This post was originally published on https://bmjopen.bmj.com